André Medici
Despite the existence of pessimistic analyzes, health in Latin America and the Caribbean has improved significantly in recent years. This improvement should be attributed overall to the regional economic development, to the massive public investment in social policies and to the social and demographic dividends characterized by increasing rates of urbanization, better educational levels (especially for women) and improvements in water and sanitation systems . Between 1990 and 2008, life expectancy at birth in Latin America increased from 68 to 73 years old, reaching higher levels than the world average (69 years) and all other developing regions.
The good performance of Latin America in extending life span is evident when compared with Eastern Europe and Central Asia countries, where life expectancy at birth in the same period increased by only one year (69 to 70 years old), starting from a higher level but getting a lower level than the Latin American Region at the end of the period. Childhood malnutrition (measured by low weight at birth) reached in 2008 only 4.5% of children under five years old - the lowest value across all Development Regions, including Eastern Europe and Central Asia. In contrast, 7.2% of Latin American children at this age group became overweight - a factor that may contribute to the early incidence of chronic diseases.
In 2010, immunization rates for DPT3 and measles reached more than 90% of the target population. The prevalence of HIV-AIDS reached only 0.5% of the population between 15 and 49 years old, lower than the world average (0.9%) and the Eastern Europe and Central Asia Regions (0.6%), although higher that of high-income countries (0.3%). The incidence of tuberculosis had fallen to 47 per 100 000 inhabitants and almost 80% of cases are reported regularly by health services, value which is surpassed only by the countries of the Middle East and North Africa, among all developing regions.
However, maternal mortality is still high in the region. In 2008 it reached 130 per 100,000 – a higher level than those in Eastern Europe and Central Asia but lower than all other Development Regions. About three-quarters of Latin American women used regularly contraceptives, which is an equivalent level of high-income countries. Thus, fertility rates were reduced dramatically and many LAC countries, achieved levels below the replacement rates.
Access to water and sanitation reached 78% of the Latin American population in 2006, a figure surpassed only by high-income countries (100%) and countries of Eastern Europe and Central Asia. Through it all, the main health problems in the Region are no longer the diseases associated with poverty (malnutrition, maternal and infant causes and transmissible diseases) and became to be the chronic conditions. Population aging is accelerating as well as the demand for more sophisticated and expensive health services and, in many countries, such as Chile, Uruguay and Costa Rica, avert infant mortality depend more of efficient and well equipped hospitals.
But better health indicators performance in Latin America in recent years is not due only to achievements in health policies. It results also from a combination of successful policies of macroeconomic stabilization, economic growth and social development implemented in the last twenty years. On the health policy side, it also responds to actions focused on improvements in primary care. This set of factors has not been able to eliminate the deep inequality that is still reflected in health indicators but turn possible sound improvements in health outcomes in the region. Among these results it could be highlighted the fast reduction of infant mortality, which has been the focus of attention of international organizations and institutions as a way to fight against poverty in the developing countries.
Reducing Infant Mortality in Latin America and the Caribbean
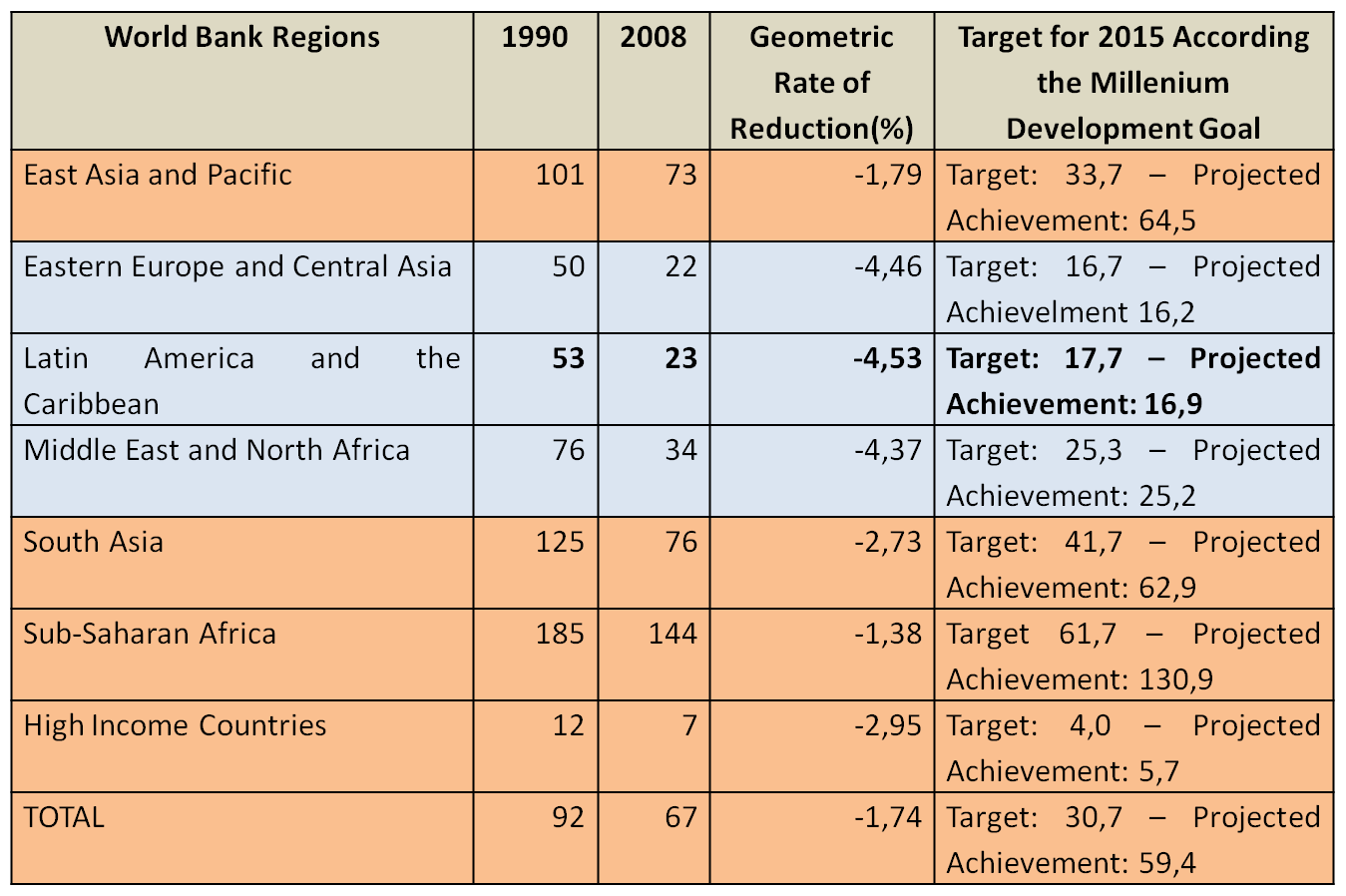
Between 1990 and 2008, the Latin America and the Caribbean Region got a fast reduction in the mortality rates for children under five years old, with an annual decrease of 4.53%. Keeping the same pace, the Region will be one of the few that will reach the Millennium Development Goal target of reducing child mortality by two thirds in 2015 (see table 1). The high-income countries, even reaching lower infant mortality rates, are not keen to achieve this target of the Millennium Development Goals.
Table 1 - Mortality Rates of Children under 5 Years Old:
1990-2008 (per 1000 live births)
The infant mortality rates in Latin America presented big disparity among countries in the early 60s’. Countries like Bolivia and Haiti, for example, in 1960 had rates close to 160 per thousand, nearly four times higher than those for Cuba, who always had lower infant mortality rates throughout the Region. Graph1 shows the infant mortality rates reduction over a half a century (1960-2010) in the five countries with higher levels of this indicator in 1960, which were Bolivia, Haiti, Peru, Guatemala and Honduras.
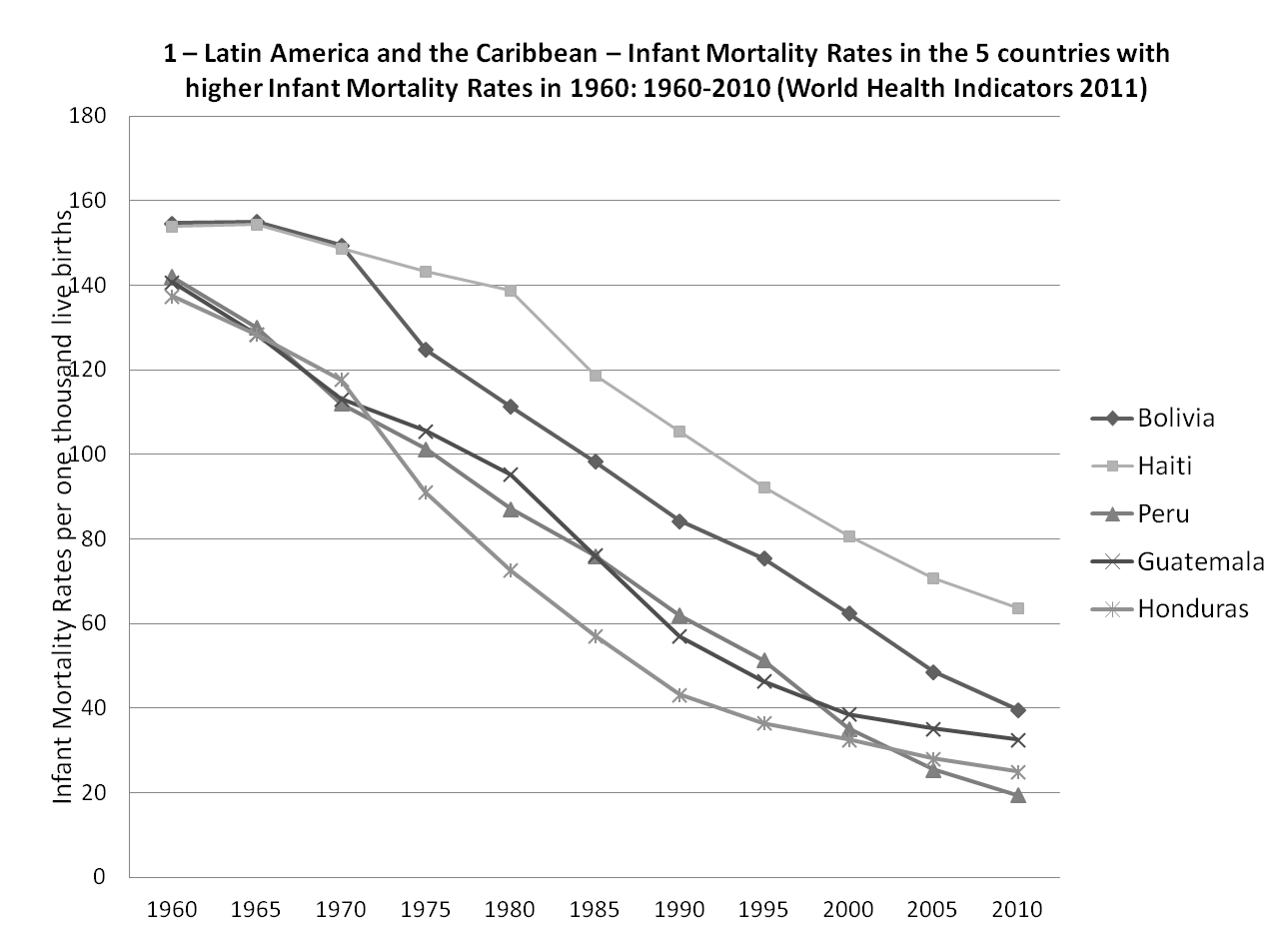
During this period, despite the fantastic reduction of child mortality in these five countries, the disparity in the level of infant mortality was increased. Haiti was the country with the lowest reduction turning from the second position in 1960 to the highest infant mortality rate in the region in 2010. Even so, the reduction was from 154 to 64 per thousand live births. Bolivia, which had the highest infant mortality rate in the region in 1960, showed a significant reduction (almost four times) - from 155 to 40 per thousand deaths in 2010. However, Peru, Guatemala and Honduras had the largest reduction, lowering their rates between four and six times, passing from 140 per thousand to levels between 20 and 35 per thousand live births.
Another way to see the evolution of infant mortality in LAC is to analyse to the countries that had the lower infant mortality rates (Cuba, Uruguay, Jamaica, Argentina and Trinidad and Tobago) in the sixities, it could be shown in Graph 2 the reduction on the infant mortality rates between 1960 and 2010.

Cuba, the country with the lowest infant mortality rate in 1960 (40 per thousand) - continued to hold this position in 2010. Its rate was reduced by almost ten times during the period, as result of a health policy focused on mother and child primary care. The infant mortality rate in Cuba in 2010 (4.4 per thousand) is similar to the countries of the European community. Countries like Argentina and Uruguay, with infant mortality rates between 50 and 60 per thousand around 1960, also suffered significant reductions in this indicator, with their rates reaching in 2010 11 and 13 deaths per thousand live births respectively. However, the same did not happen with the largest countries in the English Caribbean - Jamaica and Trinidad and Tobago. In these two countries, infant mortality rates not only decreased slightly (around half) and stagnated (Jamaica) or even increased (Trinidad and Tobago) in 1985. Another way of analyzing the infant mortality trends in the region in recent 50 years is to compare countries that delivered minor and major efforts to reduce this indicator.
Let us begin by countries that undertook major efforts. The top five are Chile, Cuba, El Salvador, Costa Rica and Peru (see chart 3). Infant mortality rates in these countries, which in 1960 presented large discrepancies (between 40 and 140 per thousand live births) began in 2010 to converge to values located between 5 and 20 per thousand live births.

In Chile, the reduction was more than 13 times, from 106 to 7 per thousand over 50 years. Chile, in 2010, reached the second highest position in the regional ranking of this indicator. In Cuba, as already noted, the reduction was ten times. In other LAC countries, such as Peru, El Salvador and Costa Rica, the reduction was also quite significant.
On the other hand, some countries apparently struggled and had worse results in the fight to reduce child mortality: they are they Trinidad & Tobago, Jamaica, Haiti, Paraguay and Bolivia (see chart number 4). Trinidad & Tobago and Jamaica - countries that in the sixties were among the five who had lower rates of infant mortality in the region, had the worst performance in reducing this indicator compared with other in the Region. Another country with equally performed poorly in this indicator is Paraguay, which even with relative high infant mortality rates in 1960, did not registered good results in the reduction of this indicator over the past 50 years.

Haiti and Bolivia are among those with the five highest infant mortality rates in the LAC Region. However, they are also among those with the worst results in the infant mortality rates in the last fifty years. Also are included as worst performers, countries such as Trinidad and Tobago and Jamaica. Although, some of the five members of the group with lower rates in 1960 were not able to maintain this position in 2010.
Accordingly, the champions in maintaining low infant mortality rates in Latin America and the Caribbean between 1960 and 2010 are Cuba (4.4), Chile (7.0), Dominica (8.1), Bahamas (8.5) and Barbados (9.8). But with the exception of Chile, all of them had relatively low rates in 1960.
What matters, therefore, is to know what could be associated with the effort made in reducing child mortality. Reviewing the last fifty years performance, it is undeniable that Chile has been the Latin American champion in the reduction of infant mortality. For this purpose, health policy makers, since the eighties, prioritized the strengthening of primary health care strategies at the local level, transfering responsabilities from central to local governments to fight infant mortality and giving technical and financial support to municipalities for this purpose.



